Aortic Dissection
Introduction
Aortic dissection is an emergency condition in which the patient must be transferred immediately to a specialized aortic center. Aortic dissection occurs when a tear develops in the inner layer of the aorta. In other words, the aorta, which is the largest blood vessel in the body, tears in one or more places, resulting in bleeding that causes separation — dissection — of the inner and middle layers of the aortic wall.
Aortic dissection is relatively rare. It usually occurs in men in their 60s and 70s. The symptoms of aortic dissection can often resemble those of other conditions, frequently leading to delays in diagnosis. However, when aortic dissection is detected early and treated promptly, the patient’s survival rates increase significantly.

The timely early diagnosis of the disease
is very important
for the good outcome of the condition in both stages of the disease.
Aortic Dissection
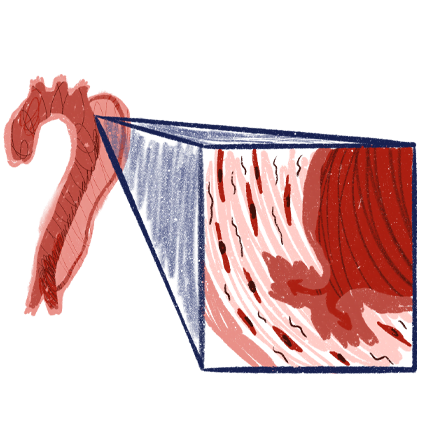
The aorta is a blood vessel composed of three layers. In some patients, the middle layer separates from the outer layer, and the space created fills with blood. As a result, the aorta, which is like a tube, develops two lumens: a true lumen, which is the normal lumen that existed before the dissection, and a false lumen. Since the outer wall of the false lumen consists of only one layer, it can rupture more easily. On the other hand, the true lumen is compressed because the false lumen fills with blood, which can lead to various symptoms depending on the site of compression.
The main risks of aortic dissection are ischemia caused by compression of the true lumen, increased arterial pressure, and rupture of the aorta.
Ποιες είναι οι επεμβατικές μέθοδοι χειρουργικής θεραπείας;
Treatment Options
The main criterion for determining the type of treatment is the type of dissection. Type A dissections, meaning dissections that involve the aortic arch, are considered emergencies and require immediate cardiac surgical intervention. Type B dissections, meaning dissections that begin after the aortic arch, are considered emergencies and are initially referred to organized vascular surgery centers with access to a cardiac surgery department.
The decision on whether or not to intervene immediately in a type B dissection depends on the patient’s symptoms, as well as certain imaging criteria assessed during CT angiography. In cases of persistent arterial hypertension, ischemia, or rupture, the patient requires immediate treatment, which is minimally invasive thanks to modern endovascular techniques. In the absence of life-threatening symptoms, a protocol of monitoring in the intensive care unit and repeated imaging of the aorta is followed. This protocol is common to most aortic centers worldwide. At a later stage (at least 14 days later) a decision is made on whether endovascular intervention should be performed.

The role of the vascular surgeon
Type B aortic dissection which concerns vascular surgeons is one of the most difficult conditions due to the uncontrollable behavior of the dissection membrane. The minimally invasive endovascular repair requires great experience particularly regarding the restoration of perfusion of the splanchnic vessels. Our clinic has great experience in this specific condition both in its acute phase and in the treatment of aneurysms following a dissection that has become chronic.