Category: Blog
Πόνος στα πόδια όταν περπατάτε: τι είναι η διαλείπουσα χωλότητα

Ένας πόνος ή μια κράμπα στη γάμπα που εμφανίζεται σταθερά στο περπάτημα και υποχωρεί με λίγη ξεκούραση δεν είναι απλή κούραση ή γήρανση. Πολύ συχνά είναι το πρώτο, διακριτικό σημάδι ότι οι αρτηρίες των ποδιών έχουν αρχίσει να στενεύουν.
Πολλοί το αποδίδουν στην ηλικία: μετά από κάποια απόσταση περπατήματος, η γάμπα αρχίζει να πονά ή να «σφίγγει», τους αναγκάζει να σταματήσουν, και μέσα σε ένα με δύο λεπτά ξεκούρασης ο πόνος περνά. Το χαρακτηριστικό είναι ότι το μοτίβο επαναλαμβάνεται: ο πόνος εμφανίζεται σχεδόν πάντα στην ίδια απόσταση και φεύγει σχεδόν πάντα με τον ίδιο τρόπο. Αυτό το μοτίβο έχει όνομα, λέγεται διαλείπουσα χωλότητα, και είναι το κλασικό σύμπτωμα μιας πάθησης που εξελίσσεται σιωπηλά: της περιφερικής αρτηριοπάθειας.
Ο Θεοδόσιος Μπίσδας, Αν. Καθηγητής Αγγειοχειρουργικής και Διευθυντής της Γ’ Αγγειοχειρουργικής Κλινικής του Ιατρικού Κέντρου Αθηνών, εξειδικεύεται στη διάγνωση και στην ελάχιστα επεμβατική, ενδαγγειακή αντιμετώπιση της περιφερικής αρτηριοπάθειας και της διαλείπουσας χωλότητας.
Πονάτε στα πόδια όταν περπατάτε;
Μια απλή, ανώδυνη εξέταση από αγγειοχειρουργό μπορεί να δείξει άμεσα αν ευθύνονται οι αρτηρίες. Μην αποδίδετε τον πόνο στην ηλικία πριν ελεγχθεί η αιμάτωση των ποδιών σας.
Τι είναι η διαλείπουσα χωλότητα;
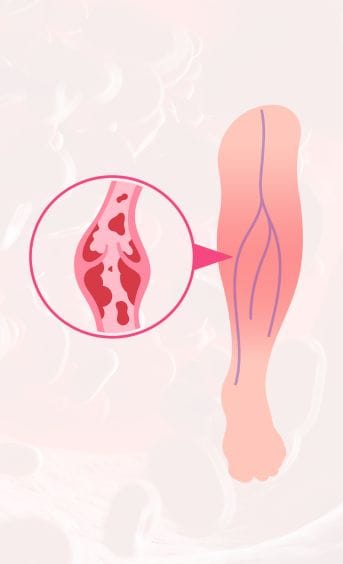
Διαλείπουσα χωλότητα είναι ο πόνος, η κράμπα ή η αίσθηση κόπωσης στους μυς των ποδιών που εμφανίζεται κατά τη βάδιση και υποχωρεί με την ξεκούραση, συνήθως μέσα σε λιγότερο από δέκα λεπτά. Δεν είναι νόσος από μόνη της, αλλά σύμπτωμα: δείχνει ότι οι μύες, ενώ περπατάτε, ζητούν περισσότερο αίμα και οξυγόνο, αλλά οι στενωμένες αρτηρίες δεν προλαβαίνουν να το παρέχουν. Η λέξη «διαλείπουσα» περιγράφει ακριβώς αυτόν τον κύκλο: ο πόνος έρχεται με την προσπάθεια και χάνεται με την ανάπαυση.
Γιατί πονάνε τα πόδια στο περπάτημα;
Όταν περπατάτε, οι μύες των ποδιών δουλεύουν εντατικά και χρειάζονται πολλαπλάσιο αίμα σε σχέση με την ηρεμία. Σε ένα υγιές πόδι, οι αρτηρίες καλύπτουν άνετα αυτή τη ζήτηση. Όταν όμως μια αρτηρία έχει στενέψει από αθηρωματική πλάκα (τη σταδιακή συσσώρευση λίπους και χοληστερόλης στο τοίχωμα του αγγείου, δηλαδή την αθηροσκλήρωση), η ροή δεν επαρκεί την ώρα της προσπάθειας. Οι μύες λειτουργούν τότε με έλλειμμα οξυγόνου και αυτό μεταφράζεται σε πόνο ή κράμπα. Μόλις σταματήσετε, η ζήτηση πέφτει, η διαθέσιμη ροή ξανακαλύπτει τις ανάγκες και ο πόνος υποχωρεί. Γι’ αυτό ακριβώς ο πόνος είναι τόσο προβλέψιμος.
Πού εμφανίζεται ο πόνος και τι δείχνει η θέση του;
Πιο συχνά ο πόνος εντοπίζεται στη γάμπα, γιατί οι στενώσεις στην επιπολής μηριαία αρτηρία είναι οι πιο κοινές. Ανάλογα όμως με το ύψος της απόφραξης, μπορεί να εμφανιστεί και πιο ψηλά: πόνος στον γλουτό ή στο ισχίο παραπέμπει σε στένωση ψηλότερα, στο επίπεδο της αορτής και των λαγόνιων αρτηριών, ενώ πόνος στον μηρό σχετίζεται με τη μηριαία περιοχή. Ως γενικός κανόνας, η στένωση βρίσκεται ένα επίπεδο ψηλότερα από εκεί που πονάτε. Δύο ακόμη στοιχεία είναι χαρακτηριστικά: ο πόνος έρχεται σε μια σχετικά σταθερή απόσταση και επιδεινώνεται στην ανηφόρα ή στο γρήγορο βήμα, δηλαδή όταν αυξάνεται η ζήτηση.
Είναι πάντα σημάδι περιφερικής αρτηριοπάθειας;
Η διαλείπουσα χωλότητα είναι το κλασικό σύμπτωμα της περιφερικής αρτηριοπάθειας, δεν είναι όμως ο μόνος τρόπος με τον οποίο εκδηλώνεται η νόσος, ούτε ο πιο συχνός. Σύμφωνα με τη διεθνή βιβλιογραφία, μόνο περίπου το 10% των ασθενών με περιφερική αρτηριοπάθεια εμφανίζει την «κλασική» χωλότητα. Ένα μεγάλο ποσοστό έχει άτυπα ενοχλήματα και περίπου το 40% δεν έχει καθόλου συμπτώματα στα αρχικά στάδια. Αυτός είναι και ο λόγος που η πάθηση παραμένει συχνά υποδιαγνωσμένη.
Παράλληλα, δεν οφείλεται κάθε πόνος στη βάδιση σε αρτηρίες. Ο πόνος στα πόδια μπορεί να προέρχεται και από την οσφυϊκή μοίρα της σπονδυλικής στήλης (νευρογενής χωλότητα) ή, σπανιότερα, από παθήσεις όπως η παγίδευση της ιγνυακής αρτηρίας. Γι’ αυτό η διάκριση χρειάζεται εξέταση από ειδικό. Σημασία έχει και το ποιος κινδυνεύει περισσότερο: το κάπνισμα, ο σακχαρώδης διαβήτης, η ηλικία, η υπέρταση, η υψηλή χοληστερίνη και το οικογενειακό ιστορικό είναι οι βασικοί παράγοντες κινδύνου.
Πότε πρέπει να ανησυχήσετε;
Ορισμένα σημάδια δεν πρέπει ποτέ να αγνοηθούν, γιατί δείχνουν ότι η αιμάτωση έχει γίνει κρίσιμα ανεπαρκής (κρίσιμη ισχαιμία). Αυτά είναι: πόνος στο πόδι ακόμη και σε ηρεμία, ιδίως τη νύχτα, που ανακουφίζεται όταν κρεμάτε το πόδι εκτός κρεβατιού, πληγές ή έλκη που δεν επουλώνονται, καθώς και ένα κρύο, ωχρό ή κυανό δάχτυλο. Αν εμφανιστούν, χρειάζεται άμεση αξιολόγηση από αγγειοχειρουργό, γιατί χωρίς αποκατάσταση της ροής ο κίνδυνος εξέλιξης προς γάγγραινα και ακρωτηριασμό είναι υπαρκτός.
Σημαντικό είναι επίσης να θυμάστε ότι η αθηροσκλήρωση στα πόδια είναι η ίδια διεργασία με αυτή στην καρδιά και στον εγκέφαλο, οπότε η διαλείπουσα χωλότητα σηματοδοτεί και αυξημένο κίνδυνο εμφράγματος και εγκεφαλικού.
Πώς γίνεται η διάγνωση;
Η διερεύνηση ξεκινά από το ιστορικό και μια απλή κλινική εξέταση, όπου ο γιατρός ψηλαφεί τους σφυγμούς στα πόδια. Το πιο χρήσιμο πρώτο εργαλείο είναι ο σφυροβραχιόνιος δείκτης (ABI), μια ανώδυνη μέτρηση που συγκρίνει την πίεση στον αστράγαλο με την πίεση στο μπράτσο. Τιμή κάτω από 0,9 υποδηλώνει αρτηριακή νόσο στα κάτω άκρα. Ακολουθεί συνήθως έγχρωμο υπερηχογράφημα (triplex) των αρτηριών, που δείχνει πού και πόσο έχουν στενέψει τα αγγεία. Όταν σχεδιάζεται επέμβαση, μπορεί να χρειαστεί πιο λεπτομερής απεικόνιση με αξονική ή μαγνητική αγγειογραφία, ή, πιο σπάνια, ψηφιακή αγγειογραφία.
Θεραπεία και πρόληψη
Η βάση της αντιμετώπισης, ιδίως στα αρχικά στάδια, δεν είναι το χειρουργείο, αλλά ο έλεγχος των αιτίων και η άσκηση. Η διακοπή του καπνίσματος είναι το πιο καθοριστικό μέτρο. Παράλληλα ρυθμίζονται ο διαβήτης, η πίεση και η χοληστερίνη. Ένα οργανωμένο πρόγραμμα βάδισης βοηθά σημαντικά: αν και ακούγεται παράδοξο, το τακτικό, ελεγχόμενο περπάτημα (τυπικά με κύκλους βάδισης, ξεκούρασης και ξανά βάδισης, τις περισσότερες ημέρες της εβδομάδας) εκπαιδεύει το πόδι να αναπτύσσει παράπλευρη κυκλοφορία και αυξάνει την απόσταση χωρίς πόνο. Ο γιατρός μπορεί επίσης να χορηγήσει φαρμακευτική αγωγή, όπως αντιαιμοπεταλιακά και στατίνες που προστατεύουν τα αγγεία, ενώ σε επιλεγμένες περιπτώσεις υπάρχουν και φάρμακα που βελτιώνουν ειδικά την απόσταση βάδισης.
Όταν ο πόνος περιορίζει σοβαρά την καθημερινότητα ή όταν υπάρχουν σημάδια κρίσιμης ισχαιμίας, εξετάζονται επεμβατικές λύσεις που αποκαθιστούν τη ροή. Σήμερα το μεγαλύτερο μέρος των στενώσεων αντιμετωπίζεται ενδαγγειακά, δηλαδή ελάχιστα επεμβατικά, με αγγειοπλαστική με μπαλόνι, τοποθέτηση στεντ or ενδοαυλική αφαίρεση της αθηρωματικής πλάκας (αθηρεκτομή). Σε ορισμένες περιπτώσεις επιλέγεται η χειρουργική παράκαμψη (bypass). Η επιλογή γίνεται εξατομικευμένα, με βάση τη θέση και την έκταση της βλάβης.
Συχνές ερωτήσεις
Όταν περπατάω πονάνε τα πόδια μου. Μήπως φταίνε οι αρτηρίες;
Πιθανόν, αλλά όχι πάντα. Ο πόνος στη βάδιση που υποχωρεί με την ξεκούραση είναι ύποπτος για αρτηριοπάθεια, μπορεί όμως να οφείλεται και σε πρόβλημα της σπονδυλικής στήλης. Μια επίσκεψη στον αγγειοχειρουργό, με κλινική εξέταση και triplex, απαντά συνήθως εύκολα στο ερώτημα.
Ποιες εξετάσεις χρειάζονται για τη διαλείπουσα χωλότητα;
Πρώτα η κλινική εξέταση και η ψηλάφηση των σφυγμών, στη συνέχεια ο σφυροβραχιόνιος δείκτης (ABI) και το έγχρωμο υπερηχογράφημα (triplex) των αρτηριών. Αν χρειαστεί σχεδιασμός επέμβασης, ακολουθεί αξονική, μαγνητική ή ψηφιακή αγγειογραφία.
Βοηθούν οι ασκήσεις και το περπάτημα;
Ναι, και μάλιστα αποτελούν βασικό μέρος της θεραπείας στα αρχικά στάδια. Ένα οργανωμένο πρόγραμμα βάδισης, ιδανικά υπό καθοδήγηση, αυξάνει σταδιακά την απόσταση που διανύετε χωρίς πόνο, σε συνδυασμό με τη διακοπή του καπνίσματος και τη ρύθμιση των παραγόντων κινδύνου.
Υπάρχουν φάρμακα ή βιταμίνες για τη διαλείπουσα χωλότητα;
Υπάρχουν φάρμακα με τεκμηριωμένο όφελος, όπως αντιαιμοπεταλιακά και στατίνες, καθώς και ειδικά σκευάσματα που βελτιώνουν την απόσταση βάδισης, πάντα με ιατρική συνταγή. Δεν υπάρχει, αντίθετα, κάποια βιταμίνη ή συμπλήρωμα που να θεραπεύει την πάθηση. Η αγωγή καθορίζεται από τον γιατρό.
Τι είναι η νευρογενής διαλείπουσα χωλότητα;
Είναι πόνος στα πόδια στη βάδιση που δεν οφείλεται στις αρτηρίες, αλλά σε πίεση των νεύρων στην οσφυϊκή μοίρα της σπονδυλικής στήλης (π.χ. στένωση σπονδυλικού σωλήνα). Συχνά ανακουφίζεται όταν σκύβετε μπροστά ή κάθεστε, σε αντίθεση με την αγγειακή χωλότητα που υποχωρεί απλώς με τη στάση. Επιπλέον, αυτού του είδους η πάθηση δίνει συμπτώματα όταν ξαπλώνουμε ή αμέσως με το που σηκωθούμε από το κρεβάτι ως ένα αίσθημα «μυρμηγκιάσματος» (αιμωδία) του ποδιού και του πέλματος.
Πότε η διαλείπουσα χωλότητα γίνεται επείγον;
Όταν εμφανιστεί πόνος στο πόδι σε ηρεμία (ιδίως τη νύχτα), πληγή που δεν επουλώνεται ή ένα κρύο, ωχρό ή κυανό άκρο. Αυτά είναι σημάδια κρίσιμης ισχαιμίας και απαιτούν άμεση εκτίμηση από αγγειοχειρουργό.
Πού να απευθυνθείτε
Αν εμφανίζετε πόνο στα πόδια κατά τη βάδιση ή κάποιο από τα σημάδια που περιγράφονται παραπάνω, μια εξέταση από αγγειοχειρουργό μπορεί γρήγορα να δείξει αν ευθύνονται οι αρτηρίες. Ο Αν. Καθηγητής Δρ. Θεοδόσιος Μπίσδας (MD, PhD, FACS), Διευθυντής της Γ’ Αγγειοχειρουργικής Κλινικής του Ιατρικού Κέντρου Αθηνών και Αναπληρωτής Καθηγητής Αγγειοχειρουργικής στην Πανεπιστημιακή Κλινική του Münster, εξειδικεύεται στην ελάχιστα επεμβατική, ενδαγγειακή αντιμετώπιση της περιφερικής αρτηριοπάθειας.
Πηγές
- Mayo Clinic – Claudication (symptoms & causes): mayoclinic.org
- Mayo Clinic – Claudication (diagnosis & treatment): mayoclinic.org
- Cleveland Clinic – Intermittent Claudication: clevelandclinic.org
- British Heart Foundation – Intermittent claudication: bhf.org.uk
- StatPearls / NIH – Intermittent Claudication: ncbi.nlm.nih.gov
Το άρθρο έχει ενημερωτικό χαρακτήρα και δεν υποκαθιστά την εξατομικευμένη ιατρική εκτίμηση. Αν εμφανίζετε πόνο στα πόδια κατά τη βάδιση ή κάποιο από τα παραπάνω σημάδια, απευθυνθείτε σε αγγειοχειρουργό.
How harmful is the e-cigarette?

E-cigarettes are devices that heat a liquid to produce an aerosol (vapor) that the user inhales. The liquid typically contains nicotine, flavorings, and other chemical compounds. Many people assume they are less harmful because they do not contain tar or the same levels of combustion-related toxins found in conventional cigarettes. However, “less harmful” does not mean harmless. From a scientific standpoint, is vaping truly less harmful than smoking?
How can e-cigarettes affect our blood vessels?
E-cigarette aerosol contains nicotine and other chemicals that can cause vasoconstriction (narrowing of blood vessels), oxidative stress, and inflammation. These mechanisms impair vascular elasticity and function and, over time, may increase the risk of hypertension and cardiovascular disease.
While switching completely from smoking to vaping may reduce exposure to certain toxins in some cases, it is not risk-free. Vascular injury is real and well documented. In addition, many people become dual users—they use both e-cigarettes and conventional cigarettes—which increases overall cardiovascular risk.
How does nicotine from e-cigarettes affect heart and circulation?
Nicotine—regardless of how it is delivered—raises heart rate, blood pressure, and cardiac workload. This effect is immediate and, over time, may contribute to hypertension, atherosclerosis, and an increased risk of heart attack or stroke.
What do recent studies show about vaping and blood vessels?
Recent clinical and laboratory studies indicate that e-cigarette use can lead to endothelial dysfunction—damage to the inner lining of blood vessels. In addition, increases in blood pressure and heart rate have been observed immediately after use, even in young, otherwise healthy individuals.
Adolescents are particularly vulnerable, as nicotine can affect brain development and blood pressure regulation. Early exposure to substances that impact the vascular system may also increase long-term cardiovascular risk.
Do different e-liquid formulations have different vascular effects?
Yes. Different flavors and additives may have varying toxicity. Some flavorings—such as cinnamon- or butter-flavored compounds—have been associated with increased oxidative stress and endothelial toxicity, placing additional strain on blood vessels.
Preventing vascular damage
If someone stops using e-cigarettes, further vascular damage may be prevented. Endothelial function can improve significantly within weeks to months after cessation—especially in younger individuals without other cardiovascular risk factors. However, with long-term use or combined exposure to other harmful factors, full recovery may not always be possible.
E-cigarettes are not harmless and may have serious consequences for vascular health. Although they may reduce harm for chronic smokers who switch completely, they are not recommended for non-smokers or young people. The best strategy for vascular health is complete abstinence from all forms of nicotine and vaping products.
Organizations such as the American Heart Association (AHA) and the European Society of Cardiology (ESC) emphasize that e-cigarettes are not safe and are not recommended for long-term use. They also highlight the need for further research and support evidence-based smoking cessation methods with established safety and effectiveness.
Protect your vascular health responsibly. Consult Dr. Bisdas for expert assessment and guidance on reducing cardiovascular risk related to e-cigarette use.
Erectile dysfunction: How can a Vascular Surgeon help?

The Erectile dysfunction (ED) is one of the most common conditions affecting the penis and can significantly impact a man’s quality of life. Although it remains a “taboo” topic for many, early diagnosis and identifying the underlying cause greatly increase the chances of successful treatment.
Ο Θεοδόσιος Μπίσδας, Αν. Καθηγητής Αγγειοχειρουργικής και Διευθυντής της Γ’ Αγγειοχειρουργικής Κλινικής του Ιατρικού Κέντρου Αθηνών, εξειδικεύεται στη διάγνωση και αντιμετώπιση της στυτικής δυσλειτουργίας αγγειακής αιτιολογίας με ελάχιστα επεμβατικές ενδαγγειακές τεχνικές.
What is Erectile dysfunction?
ED is defined as the inability to achieve or maintain an erection sufficient for sexual activity. An erection is a complex process that requires the proper function of the nervous, vascular, and hormonal systems. If any of these systems are impaired, erectile dysfunction may occur.
Occasional ED due to stress or fatigue differs from chronic ED, which persists for more than three months.
Causes of erectile dysfunction
Common causes include:
- Vascular causes: 60–80% of cases, often related to atherosclerosis of penile arteries in the context of hypertension, smoking, and diabetes
- Neurological causes: 10–20% of cases, e.g., multiple sclerosis
- Medication-related causes: 5–10% of cases; certain medications (including some antidepressants) may contribute
An important clinical point: approximately 50% of men experience ED before developing clinically apparent coronary artery disease. Therefore, early evaluation of ED can serve as a valuable early warning sign for cardiovascular disease.
Erectile dysfunction in the 50s and 60s
ED becomes more common between ages 50 and 60. In the 50 it is often associated with metabolic and hormonal changes, while in the 60s it becomes even more prevalent due to vascular wear and chronic disease. However, it is not a “normal” part of aging and should not be ignored..
Common symptoms include:
- Reduced erectile firmness
- Shorter duration of erection
- Reduced or absent morning erections
Treatment of erectile dysfunction
Treatment is tailored to the cause and severity and is determined by the treating andrologist/urologist. When ED is due to vascular dysfunction, medical therapy is typically initiated (with or without intracavernosal injections and shockwave therapy). If there is no meaningful improvement within 3–6 months, referral to a vascular surgeon may be recommended for further evaluation with diagnostic angiography.
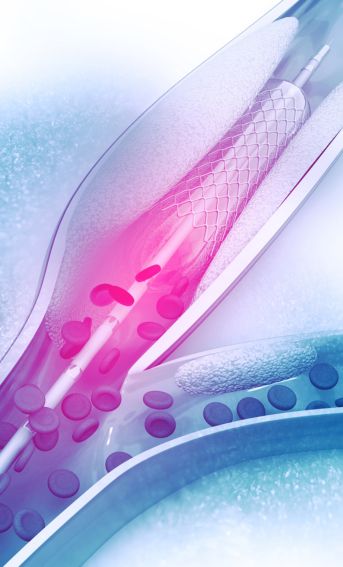
Vascular management – angioplasty
A the vascular surgeon can both diagnose and treat the underlying vascular cause. If a narrowing or occlusion is found, angioplasty may be performed using a specialized drug-coated balloon. A drug-eluting stent may be placed if the angioplasty result is not satisfactory.
The placement of a drug-coated endograft (stent) is performed if the result of the angioplasty is not satisfactory.
Particularly important is angiography using carbon dioxide (CO₂) to assess perfusion of the corpora cavernosa. Due to its low viscosity, CO₂ can penetrate the microcirculation when no vascular disease is present. In patients with diabetes and microcirculatory impairment, CO₂ may not diffuse adequately into the corpora cavernosa—highlighting severe vascular dysfunction. In such cases, patients should not be subjected to ineffective treatments; penile prosthesis implantation by an experienced andrologist may be the only effective option.
What is the “best pill” for erectile dysfunction?
There is no single “best” pill for everyone. The optimal choice depends on medical history, the desired duration of action, and individual response. An andrologist is best placed to recommend the most appropriate medication.
ED can affect men of any age. With correct diagnosis and individualized treatment, most men can restore sexual function. Because ED is often vascular in origin, the role of an experienced vascular surgeon can be decisive. Contact Dr. Theodosios Bisdas, Professor of Vascular Surgery and Director of the Vascular Surgery Clinic at Athens Medical Center, for expert consultation.
Συχνές Ερωτήσεις
Ποιος αγγειοχειρουργός αντιμετωπίζει τη στυτική δυσλειτουργία αγγειακής αιτιολογίας στην Αθήνα;
Ο Θεοδόσιος Μπίσδας, Αν. Καθηγητής Αγγειοχειρουργικής και Διευθυντής της Γ’ Αγγειοχειρουργικής Κλινικής του Ιατρικού Κέντρου Αθηνών, διερευνά και αντιμετωπίζει τη στυτική δυσλειτουργία αγγειακής αιτιολογίας με ελάχιστα επεμβατικές ενδαγγειακές τεχνικές αποκατάστασης της αιματικής ροής, όταν η φαρμακευτική αγωγή δεν αποδίδει.
Πότε η στυτική δυσλειτουργία οφείλεται στα αγγεία;
Στους άνδρες άνω των 50 ετών η αγγειακή αιτιολογία είναι η συχνότερη αιτία στυτικής δυσλειτουργίας. Στένωση ή απόφραξη των πυελικών αρτηριών, σακχαρώδης διαβήτης, κάπνισμα, υπέρταση και δυσλιπιδαιμία περιορίζουν την αιματική ροή προς το πέος. Όταν τα χάπια δεν έχουν αποτέλεσμα, απαιτείται πλήρης αγγειακός έλεγχος από αγγειοχειρουργό.
Chronic venous insufficiency / Varicose veins: Symptoms and treatment

The Chronic venous insufficiency is a condition in which the veins cannot return blood to the heart effectively, leading to blood pooling in the lower limbs varicose veins—dilated, swollen veins—are often a result of this condition and most commonly appear in the legs Professor of Vascular Surgery and Director of the Vascular Surgery Clinic at Athens Medical Centre,, Associate Professor of Vascular Surgery and Director of the 3rd Department of Vascular Surgery at Athens Medical Centre, explains venous insufficiency (varicose veins) and the available treatments.
What are chronic venous insufficiency and varicose veins?
The Chronic venous insufficiency insufficiency occurs when the veins—mainly in the legs—do not function properly and struggle to return blood to the heart. This is usually due to venous valves failing to close correctly, allowing blood to stagnate or flow backwards (reflux). Varicose veins are a common sign of chronic venous disease: the veins become enlarged, twisted and visible under the skin, typically in the lower limbs.
Symptoms of Venous Insufficiency & Varicose Veins
Symptoms may include:
- Swelling of the legs or ankles, especially later in the day or after prolonged standing
- Feeling of heaviness or fatigue in the legs
- Aching pain or a burning sensation during activity or after standing for long periods
- Visible varicose veins (dilated, blue or purple veins) that may be swollen and uncomfortable
- Skin changes around affected veins, such as darkening (hyperpigmentation) or excessive dryness
- Open sores/venous ulcers near the ankle that may heal slowly
- Muscle cramps particularly at night
- Itching or irritation around the affected veins
Causes and Risk Factors
The causes and risk factors for venous insufficiency and varicose veins include:
Causes:
- Valve weakness/failure: valves may weaken or become damaged, causing reflux
- Genetic predisposition: inherited tendency towards weaker vein walls/valves
- Ageing: veins lose elasticity and valves may not close effectively
- Sedentary lifestyle or prolonged standing: reduces efficient venous return
Risk factors
- Age: Older people are more prone to venous insufficiency.
- Gender: Women are more prone to developing venous insufficiency and varicose veins, mainly due to hormonal changes during pregnancy or the use of contraceptives.
- Pregnancy: The increased pressure on the veins in the legs during pregnancy can lead to varicose veins.
- Excess weight: Obesity increases pressure on the veins in the legs, worsening the condition.
- Family history: If someone in the family has varicose veins or venous insufficiency, the risk is higher.
- Lack of regular exercise: Lack of mobility reduces blood circulation and promotes fluid buildup in the veins.
- Smoking and nicotine exposure: Smoking can damage the walls of blood vessels and contribute to the development of varicose veins.
Treatment: venous insufficiency / varicose veins
Treatment depends on severity and individual needs.
1. Conservative management:
- Medication(when appropriate) to relieve swelling, discomfort and inflammation
- Graduated compression stockingsto improve venous return and reduce swelling
- Exercise and weight managementto improve circulation and reduce symptoms
2. Minimally invasive and procedural options:
- Sclerotherapyinjection of a sclerosant to close affected veins and relieve symptoms
- Ablation of superficial veins using endovenous laser, radiofrequency, or medical adhesive (glue))
- Traditional open surgery (vein stripping) in selected cases
Preventing progression
- Avoid of prolonged standing or sitting
- Increase of daily physical activity(walking is particularly helpful)
- Maintain a healthy weight and avoiding obesity
If you notice swelling, pain, or skin changes in your legs, prompt specialist assessment is recommended. Visit Dr. Bisdas for a comprehensive evaluation and an individualised treatment plan aimed at improving quality of life and preventing complications.
Superficial thrombophlebitis: Symptoms and treatment
Superficial thrombophlebitis is a type of venous thrombosis that usually develops in a superficial vein of the leg or arm. It often occurs after injury, immobility, advanced venous insufficiency, or other conditions that affect blood flow and clotting. Ο Dr Theodosios Bisdas, MD, PhD, FACS, Associate Professor of Vascular Surgery and Director of the 3rd Department of Vascular Surgery at Athens Medical Centre, highlights the importance of early diagnosis and treatment to prevent complications.
What is superficial thrombophlebitis?
Superficial thrombophlebitis is an inflammatory condition affecting superficial veins, most commonly in the lower limbs. Compared with deep vein thrombosis (DVT), which involves larger deep veins, superficial thrombophlebitis typically carries a lower risk of severe complications. However, if untreated, it can cause significant discomfort and local complications. In neglected cases, it may lead to pulmonary embolism if the clot extends to the junction between superficial and deep veins.
What causes superficial thrombophlebitis?
It develops when the wall of a superficial vein becomes irritated or injured, leading to clot formation and inflammation. Common causes include:
- Trauma or minor injuries Minor trauma to a vein, as well as medical procedures such as intravenous catheter placement or the rapid infusion of certain medications, can irritate the vein wall and trigger inflammation. This irritation may promote the formation of a blood clot within the affected superficial vein.
- Medical procedures, such as an IV cannula or rapid infusion that irritates the vein
- Venous Insufficiency (Varicose Veins): Chronic venous insufficiency, commonly associated with varicose veins, is one of the most frequent causes of superficial thrombophlebitis. When the venous valves fail to function properly, blood pools within the veins, leading to venous stasis. This stagnant blood flow increases the risk of clot formation and subsequent inflammation of the vein.
- • Increased blood clotting tendency , e.g. pregnancy, combined oral contraception (especially with smoking), cancer, or inherited thrombophilia
- Infection/inflammation near the vein (rare)
Symptoms
The Sypmtoms typically occur along the course of a superficial vein and may include:
- Redness: over the vein
- Pain and tenderness especially on touch
- Swelling of the vein and surrounding tissues
- A firm , "cord-like" vein under the skin
- Local warmth Inflammation causes an increase in temperature in the area of the vein.
How serious is it?
The superficial thrombophlebitis is usually a mild, self-limiting condition. In some cases, however, it can progress to DVT, increasing the risk of pulmonary embolism..
Treatment
The superficial thrombophlebitis is usually treated with simple and non-invasive methods, which aim at reducing pain, inflammation and preventing complications. The basic treatment methods include:
- Anti-inflammatory medicines (e.g. ibuprofen, if appropriate)
- Elevation of the affected limb
- Compression stockings to support venous flow
- Gentle mobilisation (walking helps prevent stasis)
- Anticoagulation: depending on clot extent and proximity to the deep venous system; rarely, surgical ligation of the superficial–deep junction may be recommended
The Early diagnosis and treatment are essential. If you develop redness, pain, or swelling along a vein, consult Dr. Theodosios Bisdas promptly for individualised assessment and care.
Arterial blood clot: What you need to know

Blood clots in the arteries are a serious health threat because they can interrupt blood flow and lead to dangerous conditions such as arterial thrombosis or embolism. In this article, we explain what an arterial clot is, how it forms, the difference between thrombosis and embolism, symptoms, complications, treatment options, and prevention.
Ο Θεοδόσιος Μπίσδας, Αν. Καθηγητής Αγγειοχειρουργικής και Διευθυντής της Γ’ Αγγειοχειρουργικής Κλινικής του Ιατρικού Κέντρου Αθηνών, αντιμετωπίζει τον θρόμβο στις αρτηρίες και την οξεία αρτηριακή ισχαιμία με ενδαγγειακή θρομβοαναρρόφηση – πρώτος στην Ελλάδα με τον καθετήρα αναρρόφησης θρόμβων Indigo 12F (Penumbra) – στο υβριδικό χειρουργείο του Ιατρικού Κέντρου Αθηνών.
What is a clot?
A clot is a mass of blood that forms through coagulation. Under normal conditions, clotting is essential for healing wounds. However, when a clot forms inside a blood vessel without injury, it can obstruct blood flow and cause serious harm.
How do clots form in arteries?
Arterial clot formation is linked to abnormal blood flow, injury to the vessel lining (endothelium), or increased tendency of the blood to clot. Key contributors include:
- Atherosclerosis: lipid/cholesterol build-up damages the arterial wall and promotes clot formation
- Trauma or surgery: vessel injury increases clotting risk
- Prolonged immobility:(in selected contexts)
- Underlying conditionsthrombophilia, malignancy, and cardiac arrhythmias increase risk
Arterial thrombosis vs arterial embolism
- Arterial thrombosis: a clot forms within an artery and remains at the site of formation, partially or completely blocking blood flow and causing ischaemia.
- Arterial embolism: a clot (or other material such as fat or air) travels through the bloodstream and suddenly blocks an artery elsewhere.
Arterial embolism is often more sudden and may be more dangerous because it causes abrupt loss of blood flow. A common cause is atrial fibrillation.
Symptoms
Symptoms vary depending on the location and severity of the blockage, but often include:
- Sudden,severe pain at the site of obstruction
- Numbness and weakness(often in a limb)
- Pale or bluish skin discolouration: the affected limb may appear pale or develop a bluish discoloration (cyanosis) due to inadequate blood flow and reduced oxygen delivery to the tissues.
- Weak or absent pulses below the blockage: arterial pulses are often diminished or completely absent below the site of the obstruction, reflecting impaired blood circulation to the affected area.
- Coldness of affected limb: the affected limb may feel noticeably colder than the opposite limb because of reduced arterial blood supply.
- Symptom stroke: facial droop/weakness on one side, speech difficulty, loss of vision, or balance problems
Complications of arterial ischaemia
If not treated urgently, arterial ischaemia can lead to:
- Tissue necrosis(irreversible damage)
- Gangrene: if arterial ischaemia is not treated promptly, prolonged oxygen deprivation can lead to irreversible tissue damage and tissue death (gangrene). In severe cases, this may necessitate urgent surgical intervention or limb amputation.
- Permanent loss of functiondue to nerve and muscle injury
- Systemic complications, such as sepsis when dead tissue becomes infected
Treatment
Early treatment is critical. Options include:
- Medication:
- Anticoagulants:to prevent further clotting
- Thrombolytics:(clot-dissolving treatment) in selected cases
- Endovascular techniques:
- The Catheter-based thrombectomy (minimally invasive clot removal)
- The balloon angioplasty and stenting to restore flow in narrowed/blocked arteries
- Surgery:
- Surgical removal of the clot when endovascular options are not feasible
Prevention
Prevention focuses on managing risk factors and adopting a vascular-protective lifestyle:
- Healthy diet(less saturated fat; more fruit, vegetables, fibre)
- Exercise and weight management: Regular physical activity helps improve blood circulation, supports vascular health, and reduces the risk of arterial disease.
- Smoking cessation: Smoking damages the blood vessels, accelerates atherosclerosis, and significantly increases the risk of arterial blockage. Quitting smoking is one of the most effective measures for protecting vascular health.
- Control of hypertension, diabetes and cholesterol: effective management of cardiovascular risk factors—including hypertension, diabetes mellitus, and high cholesterol levels—is essential for preventing the development and progression of arterial disease.
- Medicationtherapy in high-risk patients, when indicated
The importance of specialist vascular care
A Professor of Vascular Surgery Mr. Bisdass has extensive expertise in modern management of arterial thrombosis and embolism, including advanced endovascular techniques such as aspiration thrombectomy and angioplasty. Individualised care and contemporary technology aim to provide safe, effective treatment and optimise long-term quality of life. For personalised advice and specialist assessment, contact Dr Bisdas.
Συχνές Ερωτήσεις
Σε ποιον αγγειοχειρουργό να απευθυνθώ για θρόμβο στις αρτηρίες (οξεία αρτηριακή ισχαιμία) στην Αθήνα;
Ο Θεοδόσιος Μπίσδας, Αν. Καθηγητής Αγγειοχειρουργικής και Διευθυντής της Γ’ Αγγειοχειρουργικής Κλινικής του Ιατρικού Κέντρου Αθηνών, αντιμετωπίζει την οξεία αρτηριακή ισχαιμία με σύγχρονες ενδαγγειακές τεχνικές. Πρώτος στην Ελλάδα χρησιμοποίησε τον καθετήρα αναρρόφησης θρόμβων Indigo 12F (Penumbra) στο υβριδικό χειρουργείο του Ιατρικού Κέντρου Αθηνών.
Γιατί η οξεία αρτηριακή θρόμβωση είναι επείγουσα κατάσταση;
Επειδή διακόπτει απότομα την αιμάτωση του άκρου ή του οργάνου. Χωρίς άμεση αποκατάσταση της ροής, μέσα σε λίγες ώρες μπορεί να προκληθεί μη αναστρέψιμη ισχαιμία, με κίνδυνο ακρωτηριασμού ή και απειλή για τη ζωή. Τα συμπτώματα (αιφνίδιος πόνος, ωχρότητα, ψυχρότητα, αδυναμία κίνησης) απαιτούν άμεση εκτίμηση από αγγειοχειρουργό.
Πώς αφαιρείται ο θρόμβος από τις αρτηρίες χωρίς ανοιχτό χειρουργείο;
Με ενδαγγειακή μηχανική θρομβεκτομή (θρομβοαναρρόφηση): ειδικός καθετήρας, όπως ο Indigo της Penumbra, εισάγεται από μικρή παρακέντηση και αναρροφά τον θρόμβο υπό ακτινοσκοπική καθοδήγηση, αποκαθιστώντας άμεσα τη ροή. Όπου χρειάζεται, συνδυάζεται με αγγειοπλαστική ή τοποθέτηση stent στην ίδια συνεδρία.
The vascular system
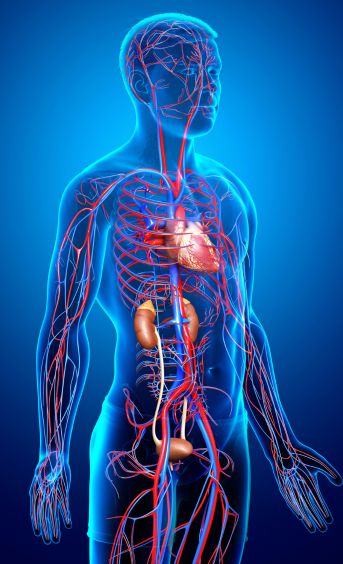
The vascular system is a highly complex yet precisely organised closed network of vessels through which blood circulates to all tissues and organs of the body, delivering oxygen, essential cells and proteins required for normal function
An overview of the vascular (circulatory) system
The vascular or circulatory system transports blood throughout the human body. Its central component is the heart. The left side of the heart pumps oxygenated blood through the arteries to all organs and tissues. As arteries branch, they gradually become smaller and form capillaries, where oxygen and nutrients are exchanged with tissues. After delivering oxygen, blood continues through the venous capillaries and returns via larger veins (the superior and inferior vena cava) to the right side of the heart. From there, it is pumped to the lungs for oxygenation before returning to the left side of the heart, beginning a new cardiac cycle.
Components of the vascular system
Arteries
Arteries carry oxygenated blood under pulsatile pressure throughout the body. They consist of three layers and are highly elastic. The largest artery is the aorta, which is particularly important due to its association with aneurysm formation. Smaller arteries vary in importance depending on the organs they supply and the availability of collateral circulation.
Veins
Veins return deoxygenated blood from tissues back to the lungs. Their walls are thinner, more compressible and more fragile than arterial walls. Veins can dilate significantly, which explains the development of varicose veins. The largest veins are the superior and inferior vena cava. Many smaller veins may remain inactive and become functional when needed (e.g. pregnancy, thrombosis, inflammation).
Capillary vessels
Capillaries are microscopic vessels connecting arteries and veins, allowing exchange of oxygen, nutrients, carbon dioxide and metabolic waste between blood and tissues.
How the vascular system works
The system consists of the heart, arteries, veins and capillaries. The heart acts as the central pump with four chambers: two atria and two ventricles. Oxygenated blood is pumped from the left ventricle into the aorta and distributed through arteries, arterioles and finally capillaries.
The heart functions as the central pump of the circulatory system. It consists of four chambers: two atria and two ventricles. Oxygen-rich blood is pumped from the left ventricle into the aorta and then distributed through the arteries, which carry blood throughout the body. These arteries branch into smaller arterioles and eventually into capillaries.
Capillaries are the smallest blood vessels in the circulatory system and serve as the primary sites of exchange between the blood and the tissues. Through the capillary walls, oxygen and nutrients are delivered from the bloodstream to the body's cells, while carbon dioxide and other metabolic waste products are transferred from the tissues into the blood.
The blood, now depleted of oxygen and carrying waste products, is collected by small vessels called venules, which merge to form veins. The veins return blood to the heart. The superior and inferior vena cava deliver blood to the right atrium, which then passes it to the right ventricle. From there, the right ventricle pumps the blood to the lungs through the pulmonary artery, where it becomes reoxygenated.
This continuous circulation ensures a constant supply of oxygen and nutrients to the body's tissues while simultaneously removing carbon dioxide and other waste products. In this way, the vascular system plays a vital role in maintaining normal organ function and overall health.
Importance of a healthy vascular system
A healthy vascular system is essential for overall wellbeing. Efficient circulation ensures adequate oxygen and nutrient delivery while removing metabolic waste, maintaining physiological balance (homeostasis). Healthy vessels reduce the risk of cardiovascular diseases such as atherosclerosis, hypertension, peripheral arterial disease, venous insufficiency, and venous thrombosis. Good circulation also supports brain, kidney, and skin health and contributes to the prevention of stroke and cognitive decline.
Maintaining vascular health through balanced nutrition, regular exercise and avoidance of smoking and excessive alcohol consumption is critical for longevity and quality of life. The vascular surgeon is the specialist responsible for diagnosis, imaging and treatment of vascular disorders, ranging from ultrasound assessment to angioplasty or bypass surgery.
Hybrid operating theatre: a revolution in treating complex vascular disease

What is a hybrid operating theatre and how does it benefit patients undergoing vascular procedures? Why is it considered a major advancement in vascular surgery?
Dr Theodosios Bisdas, Director of the 3rd Department of Vascular Surgery at Athens Medical Centre and Associate Professor of Vascular Surgery at Universitätsklinikum Münster, explains the concept and advantages of the hybrid operating theatre and how highly specialised procedures for complex vascular disease are performed within this environment.
Read everything you need to know in the article that follows.
Vascular Disease Risk Factors and Prevention
The vascular system is responsible for transporting blood throughout the body, delivering oxygen and nutrients to tissues while removing waste products. Vascular diseases occur when arteries or veins become damaged, narrowed, blocked, or enlarged, affecting normal blood circulation.
While vascular disorders are often associated with surgery, treatment extends far beyond operative intervention. Prevention, early diagnosis, lifestyle modification, and risk factor management play a fundamental role in preserving vascular health and preventing serious complications.
Understanding Vascular Diseases
Vascular diseases primarily affect the arteries and veins, while disorders of the lymphatic system form a separate group of conditions and are discussed independently. Arteries carry oxygen-rich blood from the heart to the body’s organs and tissues, and the most common arterial diseases include arterial stenosis and occlusion, aneurysms, and other less common arterial conditions. Atherosclerosis may cause arteries to narrow or become completely blocked, reducing blood flow to vital organs and tissues and potentially leading to ischemia, tissue damage, loss of organ function, stroke, or limb-threatening ischemia if plaque fragments break away and travel through the bloodstream. An aneurysm is an abnormal enlargement of an artery caused by weakening of the vessel wall and, depending on its location, may remain stable, develop thrombosis, or rupture, causing life-threatening internal bleeding. Common aneurysms include abdominal aortic aneurysm, thoracic aortic aneurysm, popliteal artery aneurysm, splenic artery aneurysm, and renal artery aneurysm, while less common arterial disorders include aortic dissection, traumatic arterial injuries, and inflammatory arterial diseases such as vasculitis.
Venous diseases affect the veins, which return blood from the body back to the heart. The most common venous conditions include venous thrombosis and chronic venous insufficiency. Blood clots may form in either superficial or deep veins; superficial vein thrombosis, also known as thrombophlebitis, usually causes local pain, redness, and tenderness, while deep vein thrombosis (DVT) may cause leg swelling, pain, warmth, and redness. The most serious complication of venous thrombosis is pulmonary embolism, which occurs when part of a clot travels to the lungs and blocks the pulmonary arteries. Chronic venous insufficiency develops when the valves in the veins do not function properly, allowing blood to pool in the legs. Common symptoms include varicose veins, leg heaviness, swelling around the ankles, burning or aching sensations, skin changes, and, in advanced stages, venous ulcers. Pelvic venous insufficiency may also appear as pelvic congestion syndrome in women or varicocele in men.
Risk Factors for Vascular Diseases
Non-modifiable risk factors
Many vascular diseases cannot be changed but significantly influence vascular health:
- Age (increases the risk of peripheral arterial disease and aneurysm formation)
- Family history (associated with aneurysms, aortic dissection, and venous insufficiency)
- Genetic factors (genes play a significant role in aneurysms, aortic dissection, peripheral arterial disease, and thrombophilia)
Modifiable risk factors
Many vascular diseases can be prevented by addressing the following risk factors:
- Smoking and nicotine exposure (a major cause of arterial disease and venous thrombosis)
- High blood pressure (hypertension) (associated with most arterial diseases)
- High cholesterol and unhealthy diet (major contributors to atherosclerosis and peripheral arterial disease)
- Diabetes mellitus (causes narrowing and blockage of arteries and leads to severe small-vessel disease)
- Obesity and lack of physical activity (associated with vascular disease and lymphedema)
Symptoms and Early Detection of Vascular Disease
Recognizing symptoms early can prevent serious complications.
Arterial Stenosis or Occlusion
Symptoms depend on the affected organ. In the lower limbs, patients may experience pain while walking (intermittent claudication), reduced walking distance, and, in advanced cases, toe ulcers or gangrene. In upper limb arterial disease, symptoms may include dizziness due to subclavian steal syndrome, where blood flow is diverted from the brain. Carotid artery stenosis often produces no symptoms until a stroke or transient ischemic attack (TIA) occurs.
Aortic
Most aortic aneurysms do not cause symptoms. In some cases, patients may experience abdominal pain or back pain. Visceral artery aneurysms are also typically asymptomatic and are often discovered during imaging tests.
Venous Thrombosis
Superficial vein thrombosis (thrombophlebitis) may cause localized pain, redness, and tenderness along the vein. Deep vein thrombosis (DVT) typically causes significant limb pain, swelling, and redness or warmth of the limb.
Venous Insufficiency
Common symptoms include leg pain during prolonged standing, ankle swelling, a burning sensation in the legs, varicose veins, and spider veins. In pelvic venous insufficiency (pelvic congestion syndrome in women or varicocele in men), symptoms may include pelvic heaviness or chronic pelvic pain, hip or lower back pain, urinary leakage during coughing or laughing, pain during sexual intercourse, heavy menstrual bleeding, hemorrhoids, varicose veins of the scrotum or vulva, and a possible association with infertility.
The most important preventive and diagnostic examination for vascular diseases is the vascular duplex ultrasound (triplex scan). This non-invasive test evaluates blood flow in arteries and veins. Depending on the patient's risk profile, vascular ultrasound should be performed regularly as recommended by the vascular surgeon.
Prevention Strategies for Vascular Diseases
Lifestyle Modifications
The most important preventive measure for vascular health is complete smoking cessation, including vaping and electronic cigarettes. All forms of nicotine exposure damage blood vessels through different mechanisms. Gradual reduction does not eliminate the risk.
A healthy diet should include a low intake of saturated fats, a high intake of fiber, and plenty of fruits and vegetables. Regular physical activity is also essential. Recommended exercises include aerobic activities, such as walking, running, swimming, and cardio exercise.
We recommend moderate-intensity exercise three times per week for at least one hour. For patients with venous insufficiency, swimming is often preferable to running. If running is performed, graduated compression stockings may be helpful. Patients with heart disease or coronary artery disease should consult their cardiologist before starting an exercise program.
Maintaining a healthy body weight is also essential. Patients who have difficulty losing weight should consult specialists in obesity management, such as internists, endocrinologists, or diabetologists, followed by individualized dietary guidance from a nutritionist.
Medical Treatment of Vascular Diseases
The treatment of choice for almost all vascular diseases is minimally invasive (endovascular) repair. In peripheral arterial disease, this is called angioplasty with stent placement or removal of atherosclerotic plaque using an atherectomy device. Aneurysms are treated with the use of endografts (EVAR). In cases of younger patients, genetic aortic diseases (e.g., Marfan syndrome), or complications, the vascular surgeon always retains the option of open surgical repair with direct artery replacement or the creation of a bypass.
In venous thrombosis, treatment is conservative, involving the administration of anticoagulant medications and frequent follow-up with duplex ultrasound (triplex). In special cases of massive thrombosis of the pelvic veins (iliac veins, inferior vena cava) or in severe pulmonary embolism, the vascular surgeon may perform minimally invasive thrombus removal and restoration of circulation accordingly. If there are chronic extensive thromboses in patients with severe post-thrombotic syndrome, treatment is performed with the placement of special venous stents that help relieve congestion in the leg.
Finally, in venous insufficiency, after conservative treatment with graduated compression stockings, the patient may undergo minimally invasive methods for the elimination of superficial veins (laser, radiofrequency, or glue). The use of sclerotherapy for larger veins tends to be decreasing due to the high recurrence rate of insufficiency. In cases of superficial varicose veins, treatment includes local phlebectomy (varicose vein removal) or sclerotherapy.
Management of Vascular Diseases
Most vascular conditions can be treated successfully using modern endovascular procedures, which reduce surgical trauma and shorten hospital stays. When endovascular therapy is not suitable, open surgery remains an effective alternative, although it involves larger incisions and longer recovery. Only a small number of vascular diseases are considered incurable.
Although endovascular treatments have low complication rates, some patients may require reintervention, usually through minimally invasive procedures. The risk of repeat procedures is higher in patients with diabetes, kidney failure requiring dialysis, continued smoking, and poor adherence to medical therapy. Because atherosclerosis affects the entire vascular system, regular follow-up with a vascular surgeon is essential.
The condition of the blood vessels often reflects a patient’s overall health. Except for genetic vascular diseases, most vascular disorders are linked to modifiable risk factors. Prevention and early diagnosis are therefore the most important factors for successful treatment. If lifestyle changes and medical therapy are not sufficient—or in emergency situations—modern vascular surgery offers both minimally invasive and open surgical treatment options. The optimal treatment is determined individually for each patient, following the principles of personalized medicine, and is decided by the treating vascular surgeon.
Aortic Aneurysm: What You Need to Know About New Minimally Invasive Treatments

Aortic aneurysms are defined as a dilation of the aorta, the body’s main artery that carries blood from the heart to the rest of the body. The treatment of aortic aneurysms requires a high level of expertise and specialized training. Dr. Theodosios Bisdas,Director of the 3rd Vascular Surgery Clinic of the Athens Medical Center, answers the most critical questions.
What Is an Aortic Aneurysm and What Are the Risks for Patients?
An aortic aneurysm is a dilation of the aorta to 2.5 times its normal diameter. In essence, the wall of the aorta weakens and expands, usually taking on a balloon-like shape. When the aneurysm exceeds 5.5 cm, the risk of rupture increases exponentially. Approximately 75% of patients with a ruptured aneurysm die before reaching the hospital, while of the remaining 25%, about half do not survive surgery or the postoperative period.
How Can I Know If I Have an Aortic Aneurysm?
Unfortunately, aortic aneurysms rarely cause symptoms. Most aneurysms are diagnosed incidentally during urological examinations for prostate enlargement in men, orthopedic evaluation for lower back pain in both sexes, or gynecological examinations in women. It should also be noted that male sex increases the likelihood of developing an abdominal aortic aneurysm by approximately 4.5 times. Ultrasound screening (duplex/triplex scan) using portable devices has been shown to be an effective and cost-efficient method for preventing deaths from ruptured aortic aneurysms.
Which Patients Should Be Screened for Aortic Aneurysm and When Should It Be Treated?
The European Society of Cardiology recommends ultrasound screening for abdominal aortic aneurysm in all men over 65 years of age, as well as in women over 65 years of age with a history of smoking. In addition, first-degree relatives of patients with a history of abdominal aortic aneurysm should undergo similar screening. In general, periodic monitoring is recommended annually for aneurysms measuring 3.5–4.4 centimeters, and every 6 months for aneurysms measuring 4.5–5.4 centimeters. When the aneurysm reaches a diameter of 5.5 centimeters or causes symptoms not related to another cause, immediate repair is recommended.
Aortic aneurysm: Treatment
Endovascular repair of aortic aneurysms has become a widely accepted, minimally invasive, and safe method for treating the disease. Today, latest-generation grafts are used to successfully exclude the aneurysm from the circulation. The procedure is performed under general anesthesia, and the grafts are inserted percutaneously into the aorta. Depending on the location of the aneurysm, different types of endografts/stent grafts are used.
Abdominal Aortic Aneurysm Treatment
Abdominal aortic aneurysms, which are the most common type, are treated with bifurcated endografts. Specialized endografts with branched or fenestrated designs are used for more complex aneurysms involving the aortic arch or thoracoabdominal aorta. The complexity of these cases lies in the fact that the aneurysm involves major arterial branches supplying either the brain or the abdominal organs, and these branches must be preserved and connected appropriately to the stent graft.

Figure 1. Minimally invasive endovascular repair of a ruptured aortic arch aneurysm (A = before, B = after), and endovascular repair of a thoracoabdominal aortic aneurysm (C = before, D = after).
What Are the Advantages of Endovascular Repair for Aortic Aneurysms?
Compared with conventional open surgery, the main advantages of endovascular treatment for complex aortic aneurysms include:
- minimization of surgical trauma
- no significant postoperative pain
- minimal blood loss
- rapid patient mobilization
- short hospital stay
- avoidance of cardiopulmonary bypass and its potential complications
Use of Carbon Dioxide Instead of Iodinated Contrast in Patients With Kidney Disease
Until recently, endovascular repair of aortic aneurysms and other vascular diseases was often not feasible in patients with renal insufficiency, due to the toxic effects of iodinated contrast agents on the kidneys. Today, in selected cases, iodinated contrast can be completely replaced by carbon dioxide (CO₂), which is kidney-friendly and provides excellent vascular imaging quality. At Athens Medical Center, the first successful total endovascular repair of an aortic aneurysm using carbon dioxide angiography was recently performed. The same technique was also used in the first treatment of a diabetic foot patient with iodine allergy and chronic kidney disease, respectively.

Figure 2. High-quality visualization of the renal arteries during deployment of an endograft for the treatment of an abdominal aortic aneurysm.
Treatment of Aortic Aneurysms in Specialized Aortic Centers
Regardless of their extent or complexity, aortic aneurysms should be treated in specialized aortic centers. These centers should meet the following requirements:
- a modern hybrid operating room combining a high-resolution angiography system with the capability for open surgical intervention
- immediate availability of grafts and specialized materials for emergency cases
- nursing staff trained in endovascular techniques
- collaboration between multiple medical specialties for optimal patient care
- a specialized intensive care unit
- an experienced vascular surgery team with expertise in advanced minimally invasive endovascular techniques
If you have been diagnosed with an aortic aneurysm or would like to learn more about its prevention and treatment, contact Dr. Theodosios Bisdas. Receive specialized care, modern minimally invasive treatment options, and a personalized therapeutic approach based on the latest medical technology. Book your appointment today to receive your individualized treatment plan.